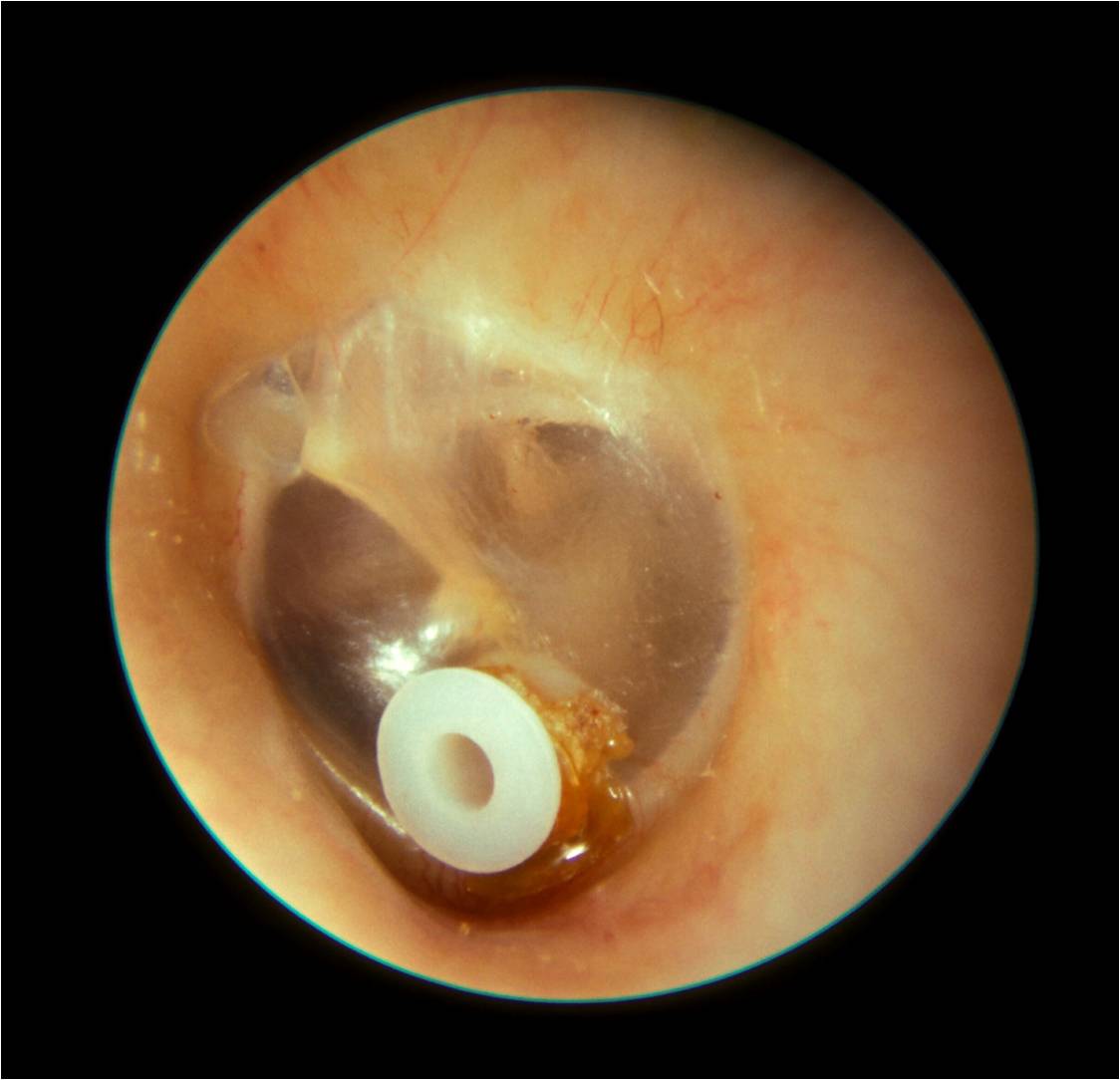
Left sided grommet (Michael Hawke MD)
Grommets
Grommets, also known as ventilation tubes (VTs) have been used as a treatment for glue ear for many years. They are small bobbin-shaped tubes which are inserted into the eardrum. Many different types are available, but the commonest ones are made of Teflon, an inert type of plastic.
The aim of grommet insertion is to allow air into the middle ear, bypassing the Eustachian tube. This influx of air improves the health of the middle ear lining and reduces inflammation, glue production and therefore improves the hearing.
Grommet insertion procedure
The procedure is usually performed under general anaesthetic as a day case, and takes 20-30 minutes (including anaesthetic time), or longer if combined with other operations. The procedure is demonstrated at http://www.youtube.com/watch?v=iFLRR1j9Ps4
Grommets typically last 6-12 months, sometimes less or more, before the eardrum skin eventually pushes them out and the hole heals over. Further grommets may be required if the glue comes back, bearing in mind that the risk of glue ear diminishes with age.
What are the risks of grommets?
It is important to realise that most children tolerate grommets very well, without complications. As discussed, they are eventually pushed out by the eardrum, after which glue ear may recur.
It is common for children to have a little clear or blood-stained ear discharge during the first few days after the procedure. This is usually not an infection, and requires no treatment apart from dry mopping of the ear with cotton wool (but not cotton buds, which should never be inserted into the ear canal). Some children may also have some ear discomfort after grommets, but this is usually short-lived. Others will have episodes of discomfort at a later stage when the ears are exposed to cold air or water- bearing in mind that the hole in the grommet allows exposure of the very sensitive lining of the middle ear.
Large studies show that the risks of other complications are low. A small number (5-10%) will suffer persistent smelly discharge from one or both ears after grommet insertions, and this may start some time after the procedure. This usually requires antibiotic ear drops (which work better than oral antibiotics). It would be useful for you to have your child’s ear(s) swabbed by your GP if this happens, prior to starting drops, to determine the bacteria responsible. Please refer to the ear drops section for specific advice about treatment of ear discharge. Repeated courses of antibiotic drops may be required. In some cases, grommets may be removed if the discharge is repeated and persistent.

Left sided eardrum perforation after grommet insertion (Michael Hawke)
In a small proportion of patients (1-2% risk after first grommet insertion), the grommet in one or both ears is pushed out by the ear drum(s), leaving a small hole (perforation). This may eventually heal, but a small operation may be required to repair the hole. This is usually delayed until ten years of age or so.
There are some other rare complications of grommets, including hearing loss, or middle ear problems as a result of eardrum skin being pushed in when the grommet is inserted (cholesteatoma).
Keeping the ears dry : washing hair and swimming
It is interesting that there is not a great deal of evidence that keeping the ears dry after grommet insertions reduces the risks of ear infections. Whilst some surgeons advise very strict water precautions, others allow patients to swim straight away without ear plugs. I typically advise that the ears should be kept dry for six weeks after grommets are inserted. This allows the middle ear lining to settle down, before exposure to water, chlorine, shampoo etc.
If parents agree (and children are cooperative), then longer water precautions are also reasonable while the grommets remain in place. I would particularly recommend this in children with repeated ear infections, or when travelling abroad and swimming in busy hotel pools which are often quite contaminated. The Keeping the Ears Dry section offers more details.
Flying and diving with glue ear and grommets
Children and adults with glue ear will struggle to "pop" their ears and equalise when flying, particularly on descent as the air pressure increases. This may be very painful. I recommend having simple painkillers available for children (paracetamol and particularly ibuprofen which works more effectively for ear pain), and measures to help the ears to equalise (water, something to eat or suck, and decongestant drops or spray eg Otrivine 30 minutes before take off and landing). Once grommets are inserted, no such problems should occur, as the ears will not need to pop (unless a grommet becomes blocked).
Diving increases the pressure on the ears far more. In glue ear, this will be extremely painful and likely to result in trauma to the eardrum and perforation. With grommets in place, high pressure water will pass through into the middle ear, again causing pain and trauma. For these reasons, swimming should be restricted to the surface.